Aortic Stenosis or Restricted Aortic Valve Opening and TAVR
Aortic stenosis is the restriction in the opening of one of the major valves of the heart. Like a door in your house not opening completely to let people out. TAVR or transcatheter aortic valve replacement is a technique to replace the restricted valve using a catheter instead of an open heart surgery.
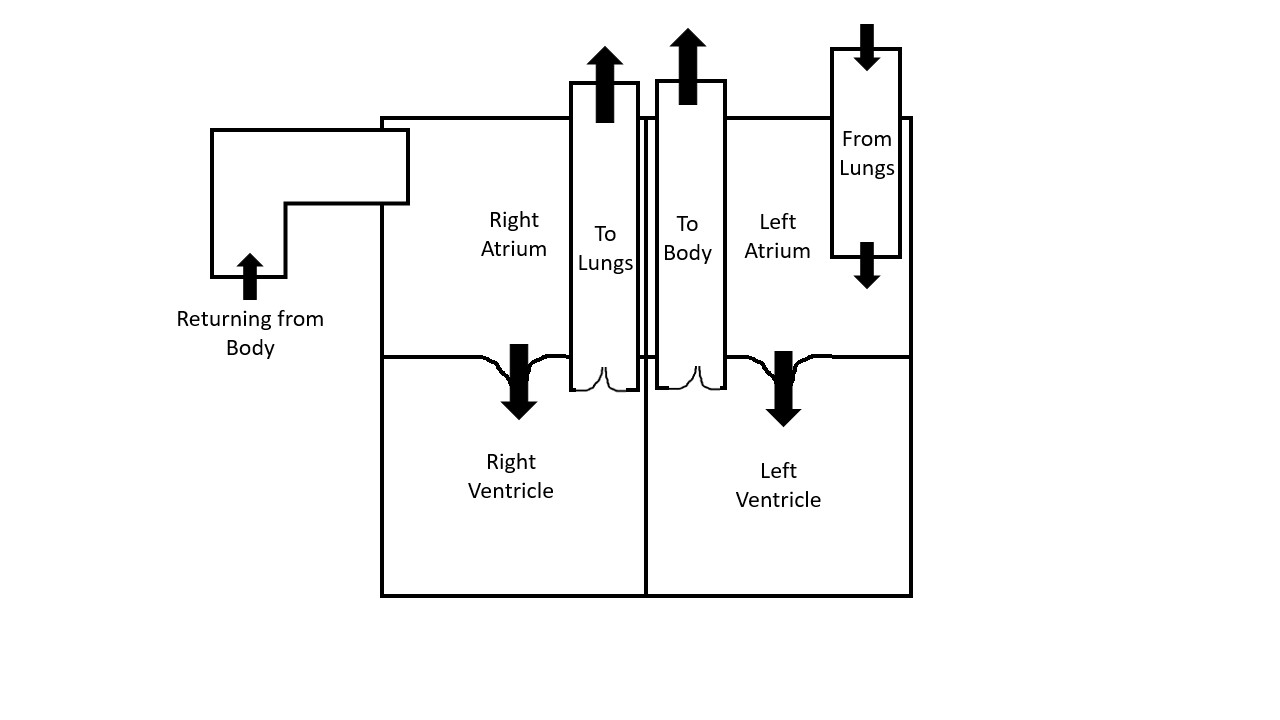
The heart has four major valves which prevent the blood from flowing back. Two valves are between the upper and lower chambers, one on the right and another on left. Two valves are between the lower chambers and arteries leading the blood out, again one on the right and another on left (figure 1). The valves prevent the blood from backing up.
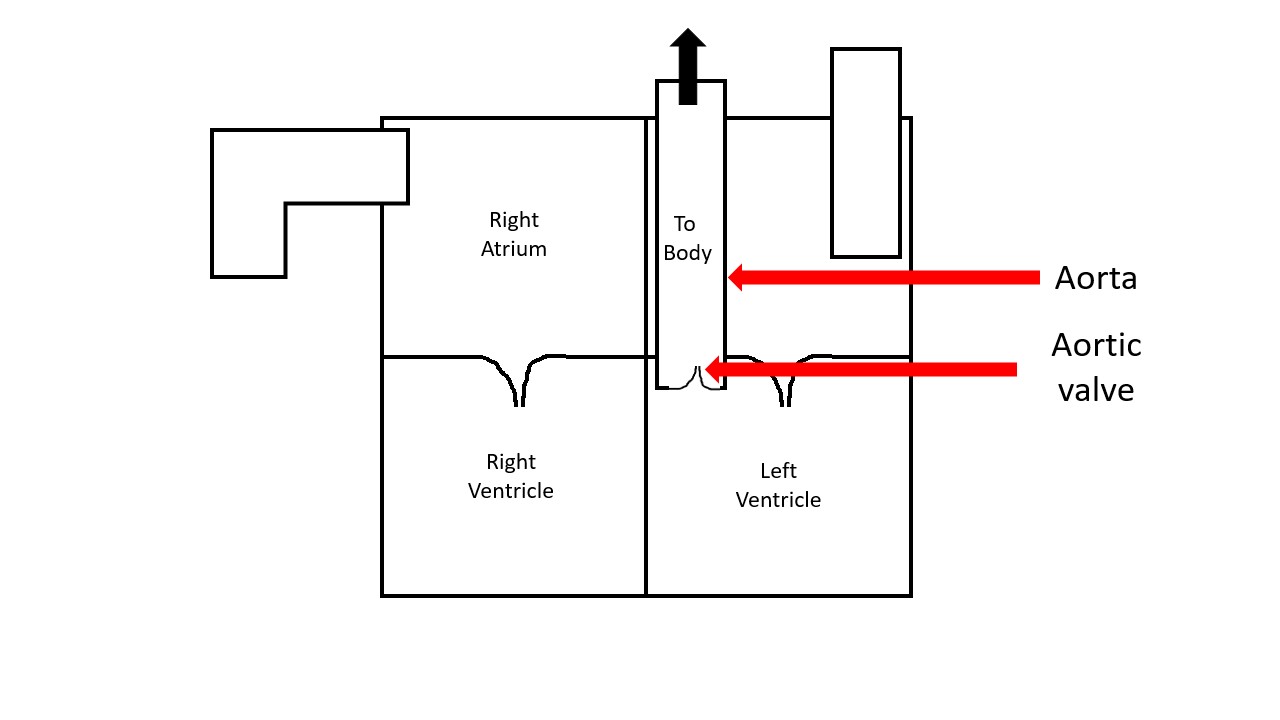
Aorta is the big artery which carries the oxygenated blood out from the left lower chamber to the body. The valve at the mouth of this aorta is called the aortic valve (figure 2).
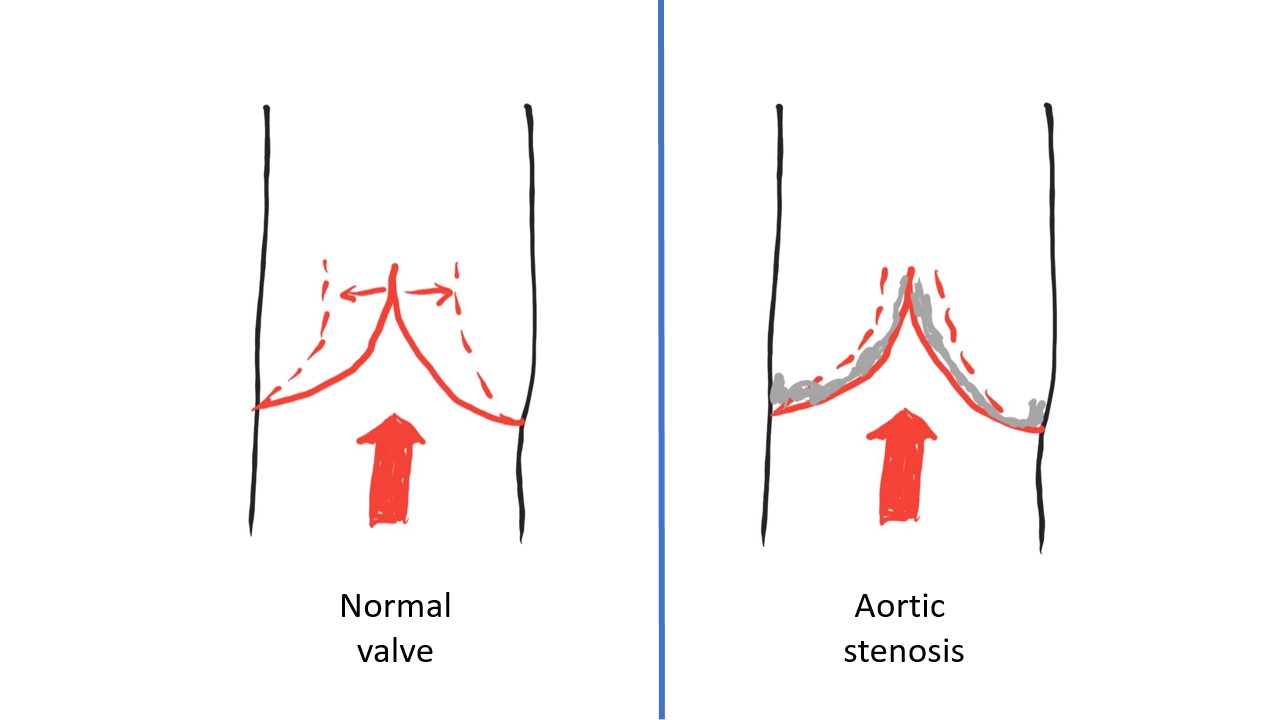
Imagine a room full of people trying to exit out of a widely open door. This is the normal heart. The door here is the aortic valve. As the door starts closing, only a few number of people can exit out at a time. This is aortic stenosis (figure 3).

The left lower chamber must work hard to push the blood out from this closing door. This takes a toll on the chamber eventually and it starts failing, resulting in heart failure. Another consequence of aortic stenosis is that less blood gets pumped out with each cycle, again due to a narrow opening in the door. Consequently, less blood reaches the organs, resulting in symptoms described below.
Risk factors:
A pre-existent valve condition or a damage in the past from infection, rheumatic heart disease or any other cause can result in narrowing in the future. A previously known malformed valve called bicuspid valve, where the valve has two leaflets instead of three, can also progress to narrowing. Calcium may build up on the valves with old age, kidney disease or in hereditary conditions, which can obstruct the opening of the valve.
Symptoms:
Early stages usually lack symptoms as the body adapts to the above changes. In later stages, symptoms such as dizziness, tiredness, syncope may happen. When the workload on the left lower chamber rises, chest pain, shortness of breath and palpitations result. The onset of symptoms usually signals progression of disease and indicate an urgency in treatment.
Diagnosis:
Early detection and treatment of aortic stenosis is the key. The manifestations can be subtle in early stages. Diagnosis requires direct visualization of the valve using ultrasound, called echocardiography or echo. Certain factors while viewing the valve decide the severity of the disease. Also important are the changes occurring to the heart as a whole as a consequence to the valve disease, including change in the heart function called ejection fraction.
The echo can be performed through a probe on the chest, which gives usable information. However, as the severity worsens or if the pictures are not clear, it becomes necessary to get the probe closer to the heart. This is done through a procedure abbreviated as TEE, where the probe is introduced into the food pipe through the mouth, just like an endoscope. The probe is now closer to the heart and can get accurate pictures of the severity.
Other modes used for diagnosis include an MRI or CT scan, however the primary mode of follow up is through an echo.
Once the door is felt to be closing, regular follow up with a cardiologist is necessary. Echo may be repeated regularly based on the severity of the disease.
Treatment:
There are largely two options for treatment. The traditional treatment option is to surgically replace the valve through an open-heart surgery. The replaced valve may be metallic or biologic such as pig/cow/deceased human valve. Metallic valves have the advantage of being durable but need blood thinners to be taken daily to prevent blood clots on the valves. Biologic valves usually do not need long-term blood thinners however they are not as durable and may need replacement after a decade. Each type of valve clearly has some advantages and the choice depends on a good discussion with the surgeon.
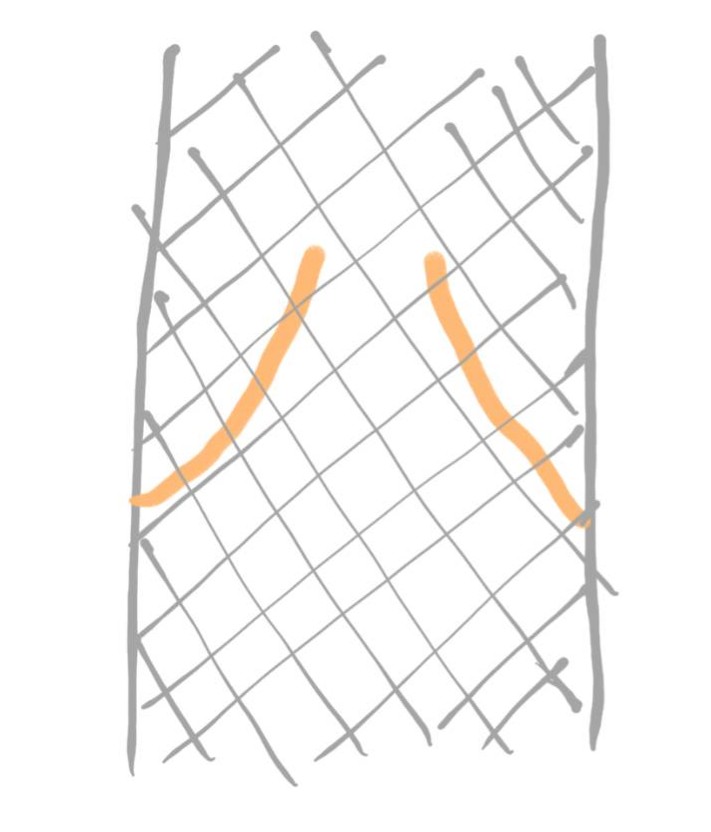
A relatively newer modality of treatment is valve replacement using a catheter. A biologic valve placed within a metallic framework is used in this technique called TAVR or transcatheter aortic valve replacement (figure 4).
In simple terms, a catheter is inserted into an artery in the leg and it is guided across the aorta towards the diseased valve. A catheter containing the metallic framework described above in a collapsed form is then guided across the valve. The framework containing a new biologic valve is then expanded across the diseased valve, squeezing it to the sides (figure 5).
Each modality of treatment has advantages over the other and the choice between these treatment options is a complex one. A good discussion with the surgeon/cardiologist is recommended.
All opinions expressed here are those of the author and not of the employer. Information provided here is for medical education only. It is not intended as and does not substitute for medical advice.
Follow on Twitter: gaurang_md

Thanks!
Very readable and ordinary person can understand…almost